Embargoed until 6pm
Media Release
22 August 2007
Report indicates that ethnic and socio-economic health inequalities are narrowing
A new report released today indicates for the first time that inequalities in health between ethnic and income groups in
New Zealand may have begun to stabilise and even decrease, the Director-General of Health Stephen McKernan says.
The report: Tracking Disparity: Trends in ethnic and socioeconomic inequalities in mortality, 1981–2004 has been jointly
published by the Ministry of Health and Otago University, Wellington. It is the fourth in the ‘Decades of Disparity’
series on ethnic and socio-economic inequalities in mortality in New Zealand.
Stephen Mckernan says in the 1980s and the 1990s inequalities in mortality (death) rates between Maori or Pacific
peoples and the European ethnic group increased steeply.
"Significantly the new report shows that between the late 1990s and the early 2000s the mortality rate ratios appear to
have stabilised and the differences in mortality rates between Maori or Pacific and European ethnic groups have
narrowed. What's more, it appears that the mortality rate ratios between low and high income groups in New Zealand are
no longer increasing as rapidly as they did in the past," Mr McKernan says.
"These findings represent a turnaround of major importance if future monitoring confirms the change in trend. Yet Maori
mortality rates remain double those of the European ethnic group, even if the difference is no longer growing. Clearly,
there is no room for complacency if we are serious about reducing inequalities in health."
The Ministry of Health has a Reducing Inequalities programme, which aims to raise awareness of health inequality and
provide District Health Boards (DHBs) and the wider health sector with skills and tools to assess, understand, and
ultimately reduce these inequalities.
"We are working closely with the four DHBs with the largest health inequalities: Northland; Lakes; Whanganui; and
Tairawhiti, to ensure that their activities are informed and focused on reducing health inequalities within their
districts.”
It will be important to continue monitoring health inequality trends over time especially now that it looks as if a
turning point may have been reached, Mr McKernan says.
Tracking Disparity: Trends in ethnic and socioeconomic inequalities in mortality, 1981–2004 will be available on the
Ministry of Health website at: http://www.moh.govt.nz/publications
ENDS
Questions and Answers
What are the key findings in the report?
Both ethnic and socio-economic inequalities in mortality appear to be no longer widening rapidly, as was the case from
the mid 1980s to the late 1990s. Instead, when measured on an absolute scale (ie the difference in mortality rates),
both ethnic (Maori: European and, to a lesser extent Pacific: European) and socioeconomic inequalities in mortality
stabilised or possibly declined between the 1996-99 and the 2001-04 periods. When measured on a relative scale (ie the
ratio of mortality rates), ethnic mortality inequalities stabilized while the socioeconomic (income) mortality gradient
continued to steepen, but much less rapidly than in the 1980s and 1990s (please see figure below).
It appears likely that the decades of increasing health inequality may be largely over. However the evidence that a
turning point has been reached is based on comparison of two timepoints only (ie comparison of 1996-99 with 2001-04 );
analysis of the 2006-09 cohort will be needed before we can be certain that a real and sustained change in inequality
trend has occurred (this analysis will only be possible in 2012).
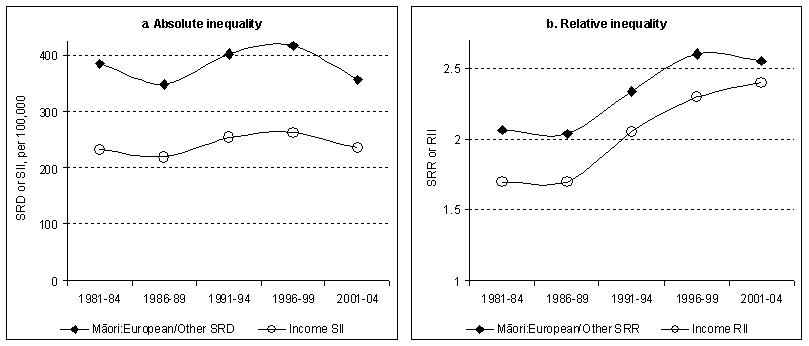
Figure Summarised presentation of estimated trends in absolute and relative inequality in all-cause mortality,
1981–2004, all ages (1-74 years) and both sexes combined
{kind=link}
Click to enlarge
Notes for figure:
The left hand chart shows absolute mortality inequality (SRD for ethnic and SII for income inequality). SRD is the age
standardised mortality rate difference. SII (slope index of inequality) is the regression-based equivalent of the SRD,
standardised for both age and ethnicity.
The right hand chart shows relative mortality inequality (SRR for ethnic and RII for income inequality). SRR is the age
standardised mortality rate ratio. RII (relative index of inequality) is the regression-based equivalent of the SRR,
standardised for both age and ethnicity.
[SII and RII are better measures of inequality than SRD and SRR respectively, as they take into account changes in the
sizes of the groups. However, these measures can be used only for groups that are ranked (eg income groups)],
While inequalities in mortality across income bands stabilised from 1996-99 to 2001-04 (on an absolute scale) for all
ages pooled (within the 1-74 age range included in the study), this was not the case for young adults (25-44 years) of
both sexes. Instead, for low income young adults there was little if any decline in mortality over the whole observation
period (1981-2004), compared with a steep decline for their high income counterparts. So for young adults the income
mortality gradient steepened steadily with no evidence of a recent slowing, unlike other age groups.
What else does the report look at?
The report also examines the contribution of different conditions to the trends in mortality disparity between Maori and
European/Other ethnic groups (Pacific and Asian ethnic groups were excluded from this aspect of the analysis due to
small numbers, resulting in insufficient statistical power), and between income bands. Cardiovascular diseases were
found to be still the major contributor to both ethnic and income mortality disparities, but are declining in
importance, with cancer (both tobacco-related and nontobacco-related) making an increasing percentage contribution over
time. Suicide has recently emerged as an important contributor to Maori – European/Other mortality inequality among male
youth.
The report further finds that socioeconomic differences (including differences in income, education, labour market
position and so on) explain at least half the Maori: European disparity in mortality (Pacific and Asian ethnic groups
were once again excluded from analysis, and for the same reason as above). Also, at least half of the widening in the
Maori : European mortality disparity from the mid ‘80s to the mid ‘90s appears to have been mediated by the
corresponding widening of social inequalities that occurred over this period (especially in relation to the labour
market).
Whether the subsequent possible narrowing in mortality disparity (when measured on an absolute scale) from 1996-99 to
2001-04 was in turn mediated (at least partially) by narrowing socioeconomic differentials cannot be determined from
this study.
Why does a person's ethnicity influence health inequalities?
Inequalities in health exist between ethnic groups and social classes in New Zealand. In all countries, socially
disadvantaged and marginalised groups have poorer health, greater exposure to health hazards, and less access to
high-quality health services. In addition, indigenous peoples and ethnic minorities tend to have poorer health. Tracking
Disparity does not identify what it is about ethnicity that accounts for its influence on health over and above its
association with socio-economic position. Other evidence (including work carried out by the Ministry using data from the
2002/03 New Zealand Health Survey) suggests that discrimination may be an important cause for ethnic inequalities in
health. Lifestyle behaviours such as smoking may explain a small part of the inequality. Genetic or biological
differences are not viable explanations for the trends in ethnic inequalities (further information is cited in the
report).
Is this the first report of its kind?
This is the fourth report in the “Decades of Disparity” series, which monitors health inequalities in New Zealand during
the 1980s, 1990s, and now the early 2000s. The first report in the Decades of Disparity series examined ethnic
inequalities in mortality, while the second investigated economic inequalities, focusing in particular on differences in
survival chances between income groups. The third report analysed interactions between ethnicity and socioeconomic
position in shaping survival chances, and quantified the extent to which ethnic inequalities in mortality are mediated
by differences in socioeconomic position. These first three reports covered the period from 1981 to 1999 – a time of
great social and economic change in our country The current (fourth) report updates the earlier series to include the
period from 2001 to 2004, thus examining trends in inequalities over nearly a quarter of a century. It is designed to
stand alone, so that readers do not necessarily need to refer back to the earlier reports in the series.
What information was used to develop the report?
Tracking Disparity: trends in ethnic and socioeconomic inequalities in mortality, 1981-2004 links mortality to census
records for New Zealanders aged 1 – 74 years for the three years following each of the 1981, 1986, 1991, 1996 and 2001
Censuses, in order to analyse ethnic and socio-economic differences in mortality rates, and to estimate how these
inequalities have trended over the 1980s, 1990s and early 2000s. This report is the fourth in the ‘Decades of
Disparity’series of monitoring reports, and updates the earlier reports.
It is important to emphasise that the apparent change in trend direction is based on a comparison of two timepoints
only: 1996-99 compared with 2001-04. We will need to wait for the next update, covering the 2006-09 period – expected in
2011 or 2012 – before we can be sure that a real and sustained turning point in ethnic and socio-economic inequalities
in health has been reached.
Why are the findings in the latest report significant?
This latest monitoring report has shown that ethnic and socioeconomic inequalities in mortality may no longer be growing
as they have been over the past two decades or so. While this is grounds for cautious optimism, these inequalities still
remain at an unacceptable level even if they are no longer rapidly increasing. The results presented in this report
should motivate the health sector and others to continue working to reduce social inequalities in health in New Zealand.
The challenge of reducing inequalities in our society continues.
Are there areas that we still need to focus on in health?
This latest monitoring report shows that we are going to have to target cancer prevention and treatment in particular,
as cancer will make an increasing relative contribution to health inequalities in future. At the same time, we must
maintain and even accelerate the dramatic progress that has been made in reducing cardiovascular disease among
disadvantaged groups – especially as we face an obesity and diabetes epidemic that is affecting these groups more
severely and could potentially wipe out the gains we have made over the past decade. Another focus of attention will
need to be young adults, for whom mortality has not declined for the low income group. Also, the recent decline in
mortality has not been as dramatic for the Pacific than for the Maori ethnic group.
Do we still need to focus on reducing inequalities?
Yes. Ethnic and socio-economic inequalities in health, and the contributions of deprivation and discrimination to these
inequalities, should continue to be monitored both nationally and at DHB level. This will enable us to see whether the
apparent turning point identified in this report is real, and if so, whether the improving trend can be not merely
sustained over the coming decade, but further accelerated. Monitoring will also illuminate which of our policies,
programmes and practices are in fact working to reduce these inequalities and their drivers – and which are not.
When will the next monitoring report be released?
The fifth monitoring report in the Decades of Disparity series, covering the 2006-09 period, should be available in 2011
or 2012.
What is the definition of mortality?
Mortality rate or death rate measures the total number of deaths per 100 000 population. All rates reported here have
been standardised for age over the 1-74 age range. Rates for income groups have been standardised for both age and
ethnicity. Ethnic rates are not standardised for income as income is a mediator, not a confounder, of the ethnicity -
mortality association.
Where can I find a copy of the report?
Tracking Disparity: Trends in ethnic and socioeconomic inequalities in mortality, 1981–2004 will be available on the
Ministry of Health website at: http://www.moh.govt.nz/publications